|
A 63 year-old man presented with a two month history of mid-back pain followed by rapidly progressive paraplegia and incontinence over 24 hours. He had a history of a nephrectomy years earlier for renal cell carcinoma. |
![]()
![]()
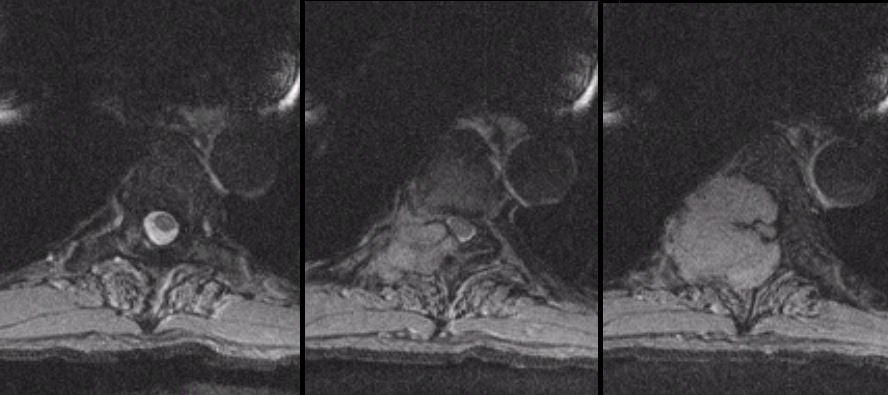
| Neoplastic Spinal Cord Compression: Axial T2-weighted MRI
scans of the thoracic spine: (Left)
T5 level; (Middle) T5-T6 level; (Right) T6 level. Note the large tumor arising from the
posterior bony elements to the right of the T6 vertebral body (right image). On
the T5 scan (left scan), note that the spinal cord is being displaced to the left. At the T6
level (right image), the spinal cord is completely encased and compressed. Decompression and biopsy
demonstrated renal cell carcinoma. Metastatic tumors that affect the spine
often begin as a metastasis to bone, especially the pedicle. As they
grow, they cause local pain. They then enlarge further and affect
the exiting nerve root at that level resulting in a clinical
radiculopathy. Only later do they grow and compress the spinal cord
or cauda equina, depending on their location. Clinical signs of
spinal cord compression typically appear acutely over hours to days.
They are a neurological / neurosurgical emergency usually requiring a
combination of high dose corticosteroids, radiation and surgical
decompression. |
Revised
11/25/06
Copyrighted 2006. David C Preston