|
A 55 year old man was brought to the ER confused. His exam showed no weakness or sensory loss. However, he could not follow any commands, and his speech was fluent with many paraphasic errors. |
![]()
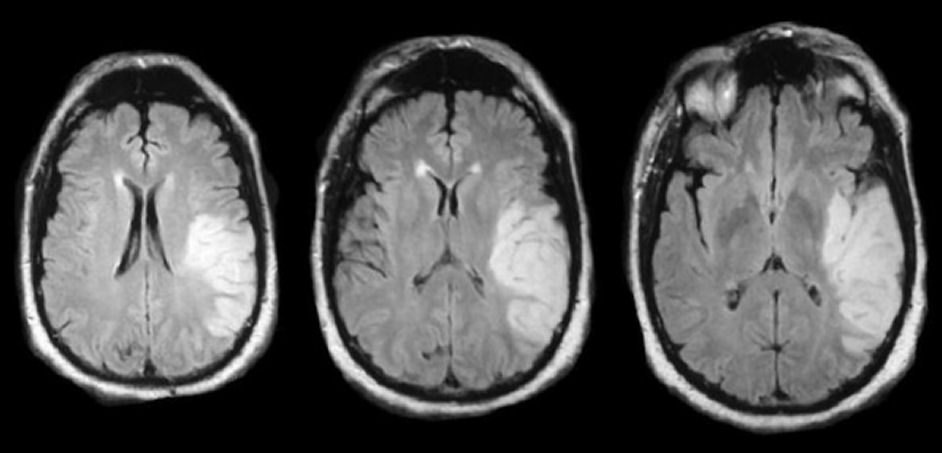
| Inferior Division Middle Cerebral Artery (MCA) Infarction: MRI Flair
Axial Scan. Note the prominent bright signal
in the distribution of the
inferior division of the left middle cerebral artery, involving the
left temporal lobe below the Sylvian fissure.
The internal carotid artery terminates in a larger MCA and smaller anterior cerebral artery. The MCA runs horizontally to the Sylvian fissure, giving off the lenticulostriate vessels. These small perforating vessels supply the basal ganglia and internal capsule. The MCA then typically bifurcates into a superior and inferior division. The superior division supplies the lateral frontal and superior parietal lobes, whereas the inferior division predominantly supplies the lateral temporal and inferior parietal lobes. The inferior division of the MCA is less commonly affected by emboli than the superior division, simply because the superior division is larger and carries more blood, and hence, it is statistically more likely for emboli to travel there. Complete infarctions on the inferior division do NOT cause any weakness or sensory loss. They typically result in a contralateral visual field deficit predominantly affecting the upper fields (i.e., "pie in the sky" deficit). With an infarct in the dominant hemisphere, there is often an associated receptive (i.e. Wernicke's) aphasia; with a non-dominant infarct, there is often behavioral disturbance and impairment of visuospatial skills (e.g., drawing, copying, dressing). It is not unusual for these patients to be misdiagnosed initially with a primary psychiatric disorder. |
Revised
11/30/06
Copyrighted 2006. David C Preston