|
A 75 year-old man developed the acute onset of a right hemiplegia and aphasia. Three days later, his right sided weakness abruptly worsened. |
![]()
![]()
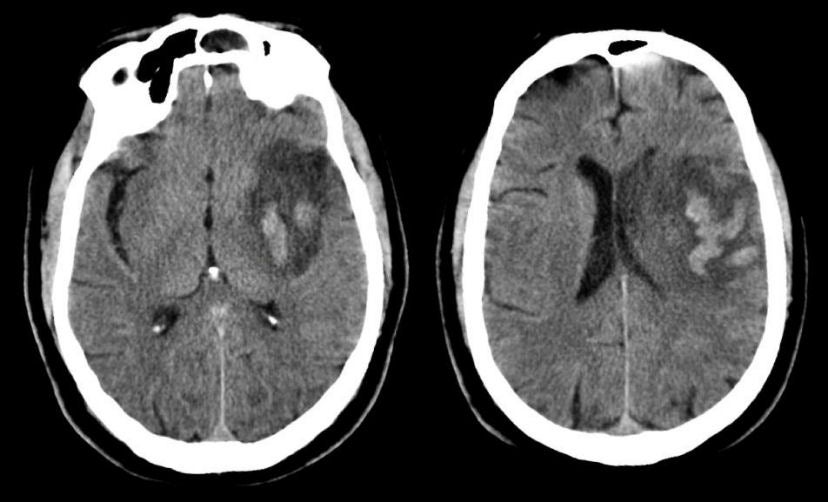
| Middle Cerebral Artery (MCA) Infarction with Secondary
Transformation:
Axial CT scans 3 days after presentation. Note the large hypodensity involving the
left middle cerebral artery territory including the deeper basal ganglia. The
involvement of the basal ganglia denotes that the blockage occurred at
the proximal middle cerebral artery stem, before the take off of the
small perforating vessels that supply the basal ganglia. Also note the hyperdensity in the basal ganglia, denoting
hemorrhagic transformation of part of the infarct. Hemorrhagic
transformation of an ischemic infarct is not uncommon and be
asymptomatic or result in neurological deterioration.
The internal carotid artery terminates in a larger MCA and smaller anterior cerebral artery. The MCA runs horizontally to the Sylvian fissure, giving off the lenticulostriate vessels. These small perforating vessels supply the basal ganglia and internal capsule. The MCA then typically bifurcates into a superior and inferior division. The superior division supplies the lateral frontal and superior parietal lobes, whereas the inferior division predominantly supplies the lateral temporal and inferior parietal lobes. Occlusions of the proximal stem of the MCA affect both the superior and inferior divisions, as well as the lenticulostriates. Complete infarctions on the distal MCA stem result in a contralateral hemiplegia (face, arm AND leg); contralateral hemisensory loss; and a contralateral visual field deficit. With an infarct in the dominant hemisphere, there is often an associated global aphasia (expressive and receptive); with a non-dominant infarct, there is often a neglect syndrome and impairment of visuospatial skills (e.g., drawing, copying, dressing). The major clinical difference between a proximal and distal MCA stem occlusion is that with a proximal lesion the leg is plegic as well. This occurs because the lenticulostriates are involved, which results in infarction of the internal capsule, which contains fibers to the leg, arm and face. |
Revised
11/29/06
Copyrighted 2006. David C Preston