![]()
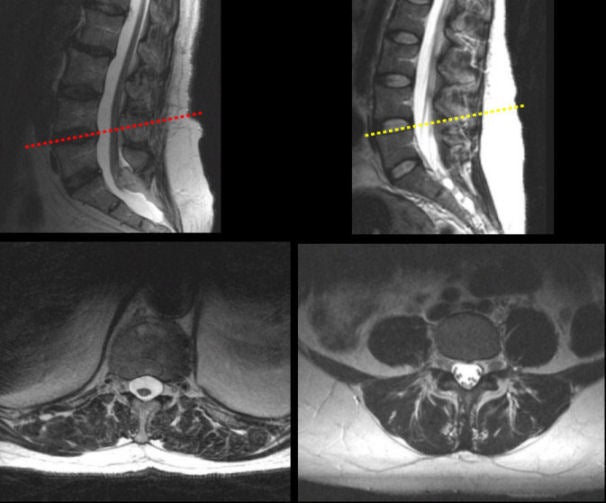
| Tethered Cord Compared to a Normal: (Top left) T2-weighted sagittal MRI in a
patient with a tethered cord and lipoma; (Bottom left) T2-weighted axial MRI at the L4-L5 level
in a patient with a tethered cord and lipoma; (Top right) T2-weighted sagittal MRI
in a normal; (Bottom right) T2-weighted axial MRI at the L4-L5 level in a normal. Note that in the patient with a tethered
cord (left images) the spinal cord terminates below L5 and can be
seen on the axial image at the L4-L5 level. In contrast, in the
normal patient (right images), the cauda equina is clearly seen on
the axial image at the L4-L5 level.
The spinal cord in adults normally terminates at the caudal level of the L1 vertebral body. A tethered spinal cord occurs when the cord becomes abnormally attached to tissue within the spinal canal, rather than floating free. This results in abnormal stretching of the spinal cord below the L1 vertebral body over time. It is more common in certain congenital disorders including myelomeningocele, lipoma or lipomyelomeningocele, diastematomyelia, dermal sinus tract, or tight filum terminale. The typical presentation is that of a slowly progressive myelopathy much like a syrinx, manifesting as a progressive gait abnormality (spastic or wide-based gait), weakness of the legs, sensory loss, and incontinence of bowel and bladder. Patients with symptomatic tethered cords often present with orthopedic deformities, including pes varus, valgus, or cavus; recurrent hip dislocations; or rotational abnormalities of an extremity or extremities. An isolated presentation of scoliosis is not uncommon. |
Revised
11/29/06
Copyrighted 2006. David C Preston