| A 22 year-old woman presented with paresthesias of the arms and legs for 2 weeks. On examination, she had a profound loss of vibration in all extremities. |
![]()
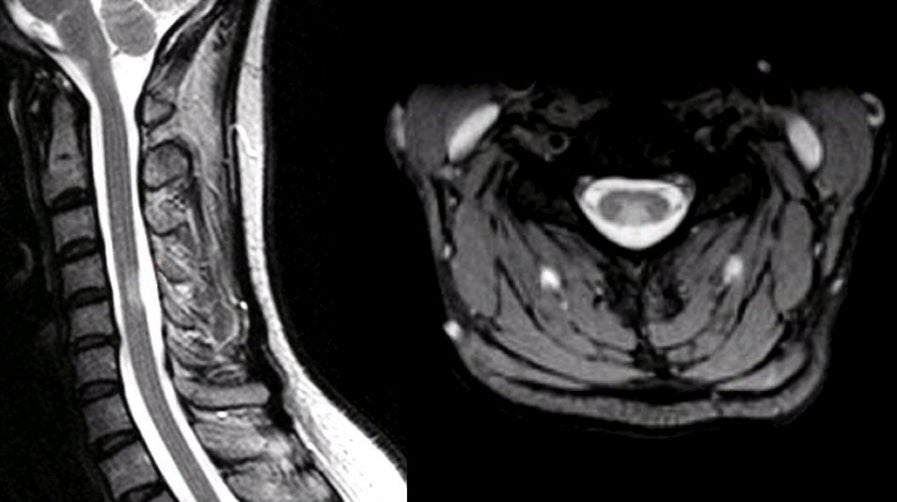
| Transverse Myelitis (TM):
(Left) T2-weighted sagittal MRI; (Right) T2-weighted axial MRI. Note
area of increased signal in the posterior aspect of the spinal cord
at the C4-5 level. The cord is not expanded. On the axial image,
note how the lesion perfectly matches the pattern of the dorsal
columns. TM is an inflammatory and demyelinating disorder of the spinal cord. Symptoms develop acutely over hours to days, resulting in partial or complete spinal cord syndromes with sensory loss, weakness and bladder/bowel disturbance below the level of the lesion. Many cases are associated with significant back or nerve root pain. Most patients make a good recovery although improvement may be delayed for weeks to months. TM is usually idiopathic and typically seen as a delayed autoimmune response to a viral or bacterial infection or an immunization. Most cases are monophasic and do not recur unless there is an underlying disorder, most often multiple sclerosis (MS) or a connective tissue disease, most notably SLE or Sjögren's syndrome. Thus, while TM may occasionally present as the first attack of MS, the diagnosis of MS should not be made on the basis of one episode of TM unless there have been previous neurological episodes separated by time and space |
Revised
11/29/06
Copyrighted 2006. David C Preston