![]()
![]()
![]()
![]()
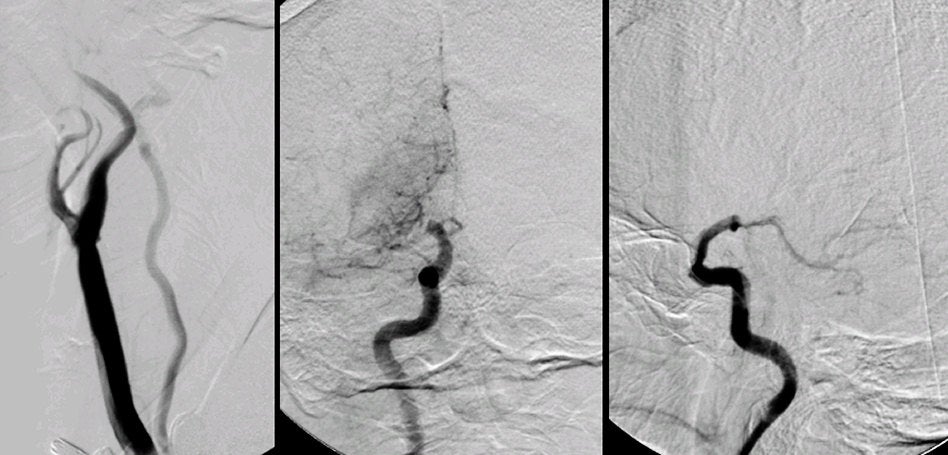
| Distal Internal Carotid Artery Infarction. (Left) Right
Common Carotid Artery angiogram; (Middle) Right Internal Carotid
Artery (ICA) angiogram,
AP view; (Right) Right Internal Carotid Artery angiogram, lateral view. On
the common carotid artery angiogram, note that the proximal internal carotid
artery is completely normal. However, reviewing the internal carotid
artery angiogram,
one notes an abrupt occlusion at the distal internal carotid artery. This is
the
typical picture of an embolus to the top of the carotid artery. Also note
the blush from increased collateral flow via the lenticulostriates.
In addition, one can see the posterior communicating artery (PComm) and some
filling of the posterior cerebral arteries (PCAs). Thus, the embolus likely
lodged distal to the take-off of the posterior communicating artery.
The internal carotid artery terminates in a larger MCA and smaller ACA. The MCA runs horizontally to the Sylvian fissure, giving off the lenticulostriate vessels. These small perforating vessels supply the basal ganglia and internal capsule. The MCA then typically bifurcates into a superior and inferior division. The superior division supplies the lateral frontal and superior parietal lobes, whereas the inferior division predominantly supplies the lateral temporal and inferior parietal lobes. Occlusions of the distal internal carotid artery affect both the superior and inferior divisions of the MCA, as well as the lenticulostriates. Complete infarctions of the distal MCA stem result in a contralateral hemiplegia (face, arm AND leg); contralateral hemisensory loss; a contralateral visual field deficit, and often a gaze preference to the ipsilateral side. With an infarct in the dominant hemisphere, there is often an associated global aphasia (expressive and receptive); with a non-dominant infarct, there is often a neglect syndrome and impairment of visuospatial skills (e.g., drawing, copying, dressing). |
Revised
11/23/06
Copyrighted 2006. David C Preston