![]()
![]()
![]()
![]()
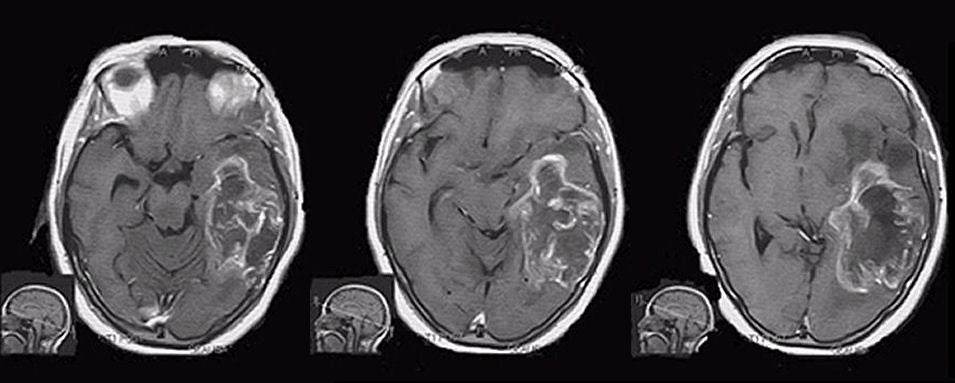
| Transtentorial Herniation:
T1-weighted with gadolinium axial MRIs. Note the midline shift and
uncal herniation, as the uncus (medial temporal lobe) is displaced against the midbrain.
In addition, note that the ambient cistern is asymmetric and larger on the left.
which occurs when the brainstem is torqued from above. If the individual
is awake when such
a massive shift of brain structures occurs (as seen on MRI), this implies that the displacement of brain structures
occurred relatively slowly, allowing time for the brain to compensate. If this
process happens quickly, such as occurs with an acute subdural hematoma, this
degree of herniation is often associated with depressed consciousness or coma.
The tentorium is a dural structure that separates the cerebrum
from the brainstem and cerebellum that lie in the posterior cranial fossa
below. The opening in the tentorium through which the brainstem,
specifically the midbrain, is connected to the cerebrum is called the tentorial
incisura. The presence of a large supratentorial mass in one
hemisphere often increases pressure from above, resulting in herniation,
whereby part of the cerebrum herniates, or is pushed through the
tentorial incisura. The structure that herniates
first is usually the uncus of the medial temporal lobe - thus the
term "uncal herniation", a subset of descending transtentorial
hernations. As the uncus
herniates, it first presses against the midbrain, resulting in an
ipsilateral third nerve palsy. Because the parasympathetic fibers
lie on
the outside of the third nerve, the first sign of uncal herniation
is usually pupillary dilatation. Further compression results in
paralysis of extraocular muscles. Because transtentorial herniation occurs most commonly from a supratentorial mass, the patient usually already has a contralateral hemiplegia. As the brainstem becomes torqued, the contralateral cerebral peduncle may become compressed against the tentorial notch (i.e., Kernohan’s notch), resulting in quadriplegia (contralateral hemiplegia from the initial lesion, ipsilateral hemiplegia from Kernohan’s notch phenomenon). As herniation proceeds, dysfunction of both cerebral hemispheres occurs, followed by dysfunction of the brainstem. As this occurs, abnormal posturing is seen. The displacement of brain structures described above illustrates the Monro-Kellie doctrine, which states that in an adult the cranial volume is a constant. The cranial contents consist primarily of brain, cerebrospinal fluid (CSF) and blood vessels. If a mass such as a hematoma, tumor or edema develops, these elements must shift to accommodate the mass. Since the cranial volume is a constant, part of the cranial contents will herniate through the tentorial incisura to make room for the mass. The opposite occurs in a patient with loss of brain mass, such as occurs after a stroke, wherein the CSF spaces often enlarge to fill the void. |
Revised
11/30/06
Copyrighted 2006. David C Preston