|
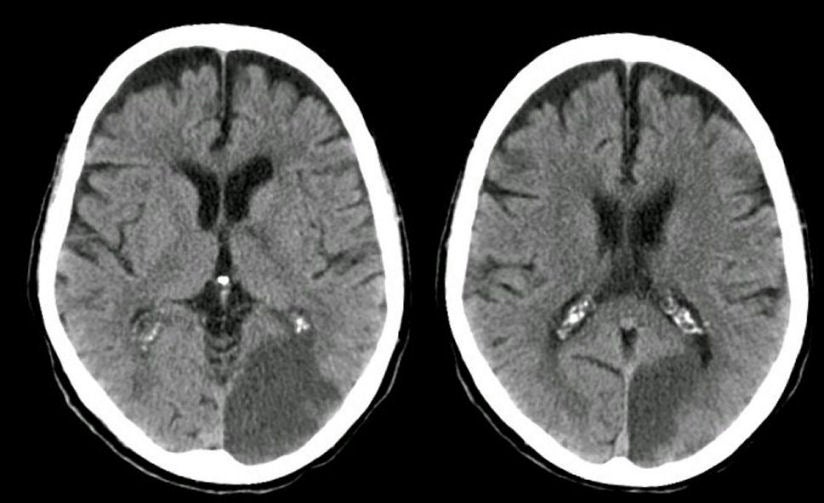
A 72 year-old woman developed the abrupt onset of difficulty seeing on the right side. |
![]()
| Posterior Cerebral Artery (PCA) Infarction:
Axial CT scans 3 days after presentation. Note the hypodensity in the left occipital lobe
in the distribution of the
left posterior cerebral artery. This syndrome is most often caused by a cardiac embolus or an embolus from an occluded or stenotic proximal vertebral or basilar artery. The basilar artery bifurcates into two PCAs at its termination, which then course around the midbrain in the ambient and quadrigeminal cisterns to supply the medial / inferior temporal lobe and the medial occipital lobe. Small perforators arise from the proximal PCAs, which supply the cerebral peduncle as well as the thalamus (the latter known as thalamoperforators). Infarctions in the territory of the PCA most often result in a contralateral hemianopsia. Other signs and symptoms depend on whether the infarction involves the thalamoperforator territory, and whether the infarction is left vs. right sided. Proximal PCA involvement results in coexistent infarction of the lateral thalamus, with contralateral hemisensory findings. Infarction of either PCA may result in impaired memory (verbal on the left; spatial on the right). In addition, left PCA lesions are sometimes associated with alexia without agraphia (patients can write, but cannot read what they have written); transcortical sensory aphasia (a receptive aphasia similar to Wernicke's aphasia except that repetition is relatively spared); and Gerstmann's syndrome (a combination of acalculia, finger agnosia, agraphia, and right/left confusion). With right sided PCA lesions, patients may have a visual neglect. They may also have prosopagnosia, an inability to recognize familiar faces. |
Revised
11/23/06
Copyrighted 2006. David C Preston