|
A 55 year-old man developed progressive pain, weakness and paresthesias of the legs while walking or standing. Only sitting would relieve the symptoms. His neurological exam was normal other than depressed ankle reflexes. |
![]()
![]()
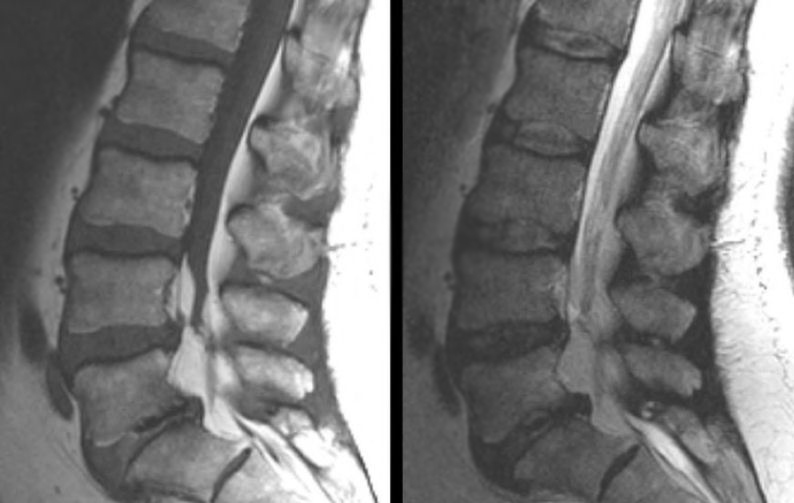
| Epidural Lipomatosis: (Left)
T1-weighted sagittal MRI of the
lumbar spine; (Right) T2-weighted sagittal MRI of the lumbar spine.
Although there is degenerative disk disease, especially at L5-S1,
the major finding is the massive amount of epidural fat that
compresses the thecal sac from L4 and below. On MRI imaging, fat is bright
on both T1- and T2-weighted images (although brighter on T1-weighted). Since CSF is also
bright on T2-weighted images, T1-weighted images allow for easy differentiation
between fat (which is bright on T1-weighted images) and CSF (which
is dark on T1-weighted images). Epidural lipomatosis refers to an abnormal accumulation of fat in the epidural space within the spine, which generally occurs in the lumbar and sacral regions. It is most often seen in the context of corticosteroid therapy, endocrinopathies (e.g. ectopic ACTH secretion), or significant obesity. Epidural steroid injections have also been implicated as an etiologic factor. Most patients present with back pain and lower extremity weakness, similar to patients with degenerative spinal stenosis. Depending on the etiology, epidural lipomatosis may resolve after reduction or cessation of the causative factor, such as cessation of steroid therapy, bilateral adrenalectomy, or weight reduction. Multilevel laminectomy with debulking of the epidural fat produces neurological improvement in more than 75% of cases. |
Revised
11/22/06
Copyrighted 2006. David C Preston