|
A 35 year-old man presented with headaches and gait imbalance. He had been hospitalized for six weeks as a child for meningitis. |
![]()
![]()
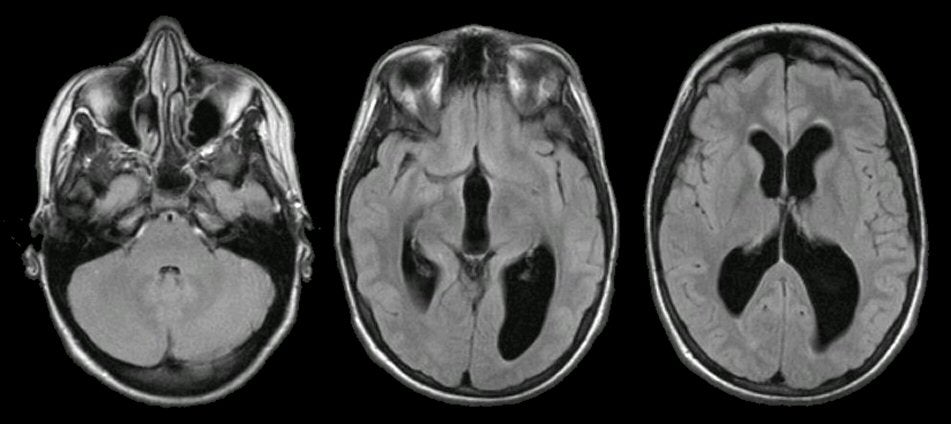
| Non-Communicating Hydrocephalus: Flair axial MRI images.
Note the prominent enlargement of the lateral and third ventricles
in the setting of a normal sized fourth ventricle (left image). This
pattern is one of non-communicating (obstructive) hydrocephalus,
which occurs from impaired drainage through the cerebral aqueduct
which connects the third and fourth ventricles. This picture differs
from communicating hydrocephalus wherein all the ventricles are
enlarged. Note also that the sulci are relatively effaced (i.e.
small), which excludes the possibility that the enlarged ventricles
are simply due to cerebral atrophy (i.e., hydrocephalus ex vacuo).
In this case, the hydrocephalus likely resulted from scarring in the
cerebral aqueduct as a consequence of his meningitis as a child. Hydrocephalus is recognized as enlarged ventricles out of proportion to the amount of cerebral atrophy. Non-communicating (obstructive) hydrocephalus occurs when the ventricular system is not in continuity with the subarachnoid space. Most often, the site of the blockage in non-communicating hydrocephalus is at the cerebral aqueduct, but rarely can occur at the foramen of Monro, the third ventricle, or the outlet of the fourth ventricle. Acute non-compensated, non-communicating (obstructive) hydrocephalus is a neurosurgical emergency as the non-compensated hydrocephalus results in a progressive increase in intracranial pressure, which if left unchecked will result in herniation and brain death. It is potentially treatable by shunting. |
Revised
11/29/06
Copyrighted 2006. David C Preston