|
A 32 year-old man with a ventriculoperitoneal shunt presented with headaches and progressive confusion. |
![]()
![]()
![]()
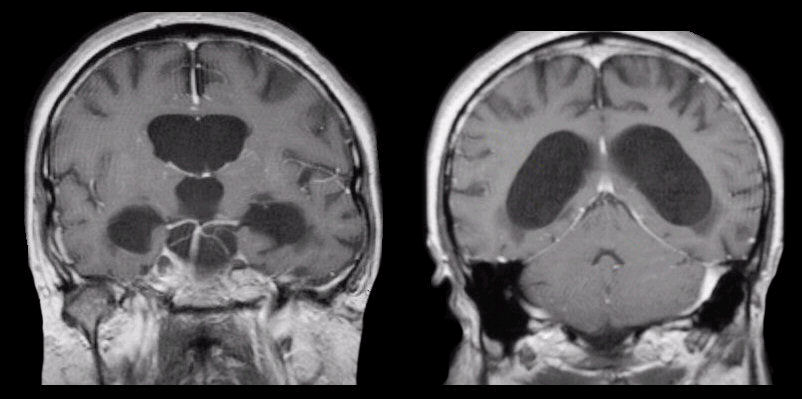
| Non-Communicating Hydrocephalus:
T1-weighted with gadolinium coronal MRIs.
Note the prominent enlargement of the lateral and third ventricles
in the setting of a normal sized fourth ventricle. This pattern is
one of non-communicating (obstructive) hydrocephalus, which occurs
from impaired drainage through the cerebral aqueduct which connects
the third and fourth ventricles. This picture differs from
communicating hydrocephalus wherein all the ventricles are enlarged.
This patient had chronic hydrocephalus from an episode
of head trauma during childhood, which had been
successfully treated with a shunt. However, when the shunt malfunctioned, acute
hydrocephalus developed, resulting in marked symptoms. Shunt malfunction is a common
cause of acute hydrocephalus, which requires immediate neurosurgical
intervention, to reduce the pressure. Also note the incidental finding of a well seen basilar artery and
posterior cerebral and superior cerebellar arteries in the scan on
the left. Hydrocephalus is recognized as enlarged ventricles out of proportion to the amount of cerebral atrophy. Non-communicating (obstructive) hydrocephalus occurs when the ventricular system is not in continuity with the subarachnoid space. Most often, the site of the blockage in non-communicating hydrocephalus is at the cerebral aqueduct, but rarely can occur at the foramen of Monro, the third ventricle, or the outlet of the fourth ventricle. Acute non-compensated, non-communicating (obstructive) hydrocephalus is a neurosurgical emergency as the non-compensated hydrocephalus results in a progressive increase in intracranial pressure, which if left unchecked will result in herniation and brain death. It is potentially treatable by shunting. PCA = posterior cerebral artery, SCA = superior cerebellar artery. |
Revised
12/02/06
Copyrighted 2006. David C Preston