|
A 52 year-old man with a history of alcohol abuse was brought in by his family for confusion. On examination, he had bilateral sixth nerve palsies and difficulty with upgaze. |
![]()
![]()
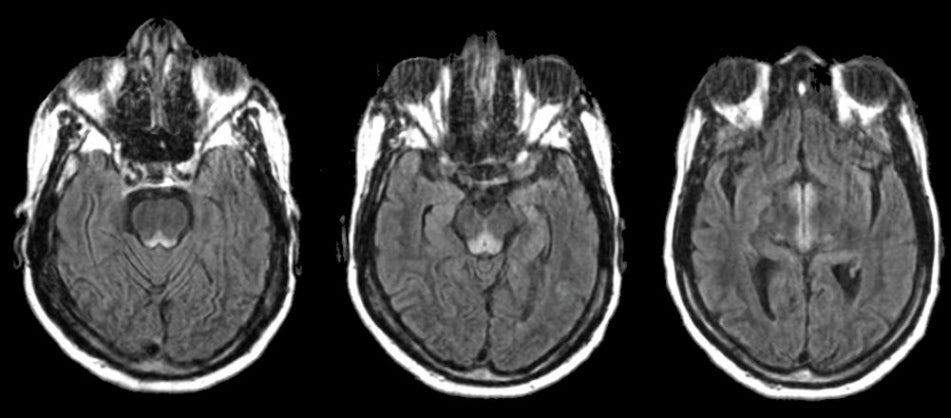
| Wernicke's Encephalopathy:
Flair axial MRI scans. Note the abnormal signal in the periaqueductal gray matter of the
upper pons and midbrain
(left and middle images),
as well as in the medial hypothalamus (right image),
changes typical of Wernicke's encephalopathy.
Wernicke's encephalopathy results from thiamine deficiency, and constitutes a medical emergency. Left untreated, coma and death may ensue within days. It is seen most often in alcoholics, but also occurs in the setting of poor nutrition from many other causes, including bariatric surgery, morning sickness associated with pregnancy, and intractable vomiting associated with chemotherapy. The classic triad of Wernicke's encephalopathy includes mental state changes, ataxia, and ophthalmoplegia (especially CN VI). However, all three components may not be present initially. In other cases, Wernicke's encephalopathy may present as seizures, including status epilepticus, visual loss, or coma. The eye findings in Wernicke's encephalopathy include gaze palsies, partial palsies of cranial nerves III, IV, or VI, and nystagmus. |
Revised
11/30/06.
Copyrighted 2006. David C Preston