Seeing inside: CWRU makes pioneering contributions to medical imaging through history
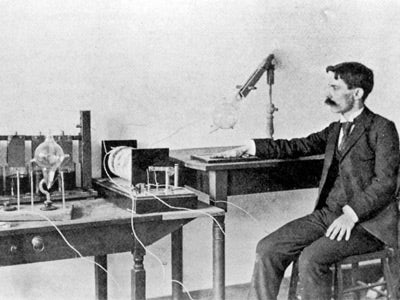
When Dayton C. Miller, PhD (HON 1927), learned invisible light rays could pass through objects and leave images on film, he decided to experiment.
In the winter of 1896, the Case School of Applied Science physics professor took X-rays of his body in sections on glass plates—and then put the plates together to create the first-ever full-body X-ray image.
The value of such images became clearer after Miller was asked to X-ray a patient’s broken arm and detected that the limb had not been properly set.
Today nearly every medical diagnosis relies on imaging: MRIs, CT scans, ultrasounds—all developed since Miller and others began to peer within.
“Fundamentally, being able to visualize something inside the human body changed the way that we practice medicine,” said Agata Exner, PhD (CWR ’98; GRS ’00, ’03, biomedical engineering), director of the interdisciplinary Case Western Reserve University Center for Imaging Research, the Henry Willson Payne Professor of Radiology at the School of Medicine and a professor of biomedical engineering.
For decades, CWRU has had a groundbreaking impact in medical imaging research by capitalizing on its unique collaborative ecosystem that unites engineering, basic sciences, medicine and primary clinical partners at University Hospitals (UH) and Cleveland Clinic, Exner said. Their collective culture of innovation, strengthened by partnerships with CWRU startups and both local and international manufacturers, drives rapid translation of technology from research to clinical use.
Innovation in action
In the 1970s and early 1980s, university and UH faculty-physicians pioneered new procedures. John Haaga, MD, performed the first image-guided biopsy of a tumor, Exner said, while Martin Resnick, MD, performed the first ultrasound-guided biopsy of a prostate tumor—laying the groundwork for minimally invasive, radiology-guided cancer screenings and treatments.
Today, the university and the Case Comprehensive Cancer Center have faculty researchers—including Exner, who also is co-leader of that center’s Cancer Imaging Program—at the forefront of the field. They are developing advances in both imaging and contrast agents that work in tandem to better diagnose and more precisely treat tumors. That includes making difficult-to-see brain tumors easier for surgeons to completely remove. Others are developing artificial-intelligence models to integrate imaging with other clinical data to aid diagnoses and predict disease risk.
But perhaps the most impactful and enduring imaging work is a partnership launched more than 40 years ago that has helped improve MRI machines used around the world—as well as the ability of clinicians to test some cancer therapies because they literally can see sooner and better whether those therapies are working or not.
Since 1984, CWRU and UH have partnered with Siemens, a global medical-technology company. And their collaboration, UH said last summer in a statement, “continues to shape the science and practice of medicine.”
A key element: CWRU and UH are sent Siemens’ state-of-the-art MRI equipment, long before it is available commercially.
“We get access before the rest of the world, and we can also work with the company to commercialize the technology we develop,” said Mark Griswold, PhD, who holds the Pavey Family Professorship in Innovative Imaging - Revolutionizing the Worlds of Education and Medicine in radiology at the medical school and also is a professor of biomedical engineering and physics, and a member of the cancer center.
Griswold and Jeffrey Sunshine, MD, PhD, chief medical information officer at UH and a professor of radiology at the medical school, lead the CWRU-UH side of the collaboration, which UH said has garnered more than $100 million in National Institutes of Health funding in the last 20 years and $15 million in Siemens-sponsored research, and resulted in more than 130 U.S. patents and 30 international ones generated by faculty, staff and students.
Sunshine sees an even bigger footprint: Technologies developed through the collaboration have shaped multiple products used worldwide, impacting the care of over 100,000 patients daily.
The partnership’s day-to-day work is best seen in the swirl of activity in a basement laboratory in University Hospitals’ Bolwell Building, deliberately situated amid clinical MRI imaging rooms where patients undergo scans.
Broadening Impact
In just the last decade, CWRU faculty who are members of the campus Center for Imaging Research have conducted research that led to:
Here, radiology clinicians bump elbows, literally, with biomedical engineers, physicists and mathematicians. Graduate students and postdoctoral researchers from different research groups sit at clusters of desks, developing new methods for collecting MRI data, refining techniques or analyzing data from clinical trials.
“In our lab meetings, we have all the people who work on the tools, from the theory to the hardware, and the clinicians who make decisions about clinical practice in a major hospital,” said postdoctoral associate Reid Bolding, PhD (CWR ’20; GRS ’26, physics).
Such collaboration and conversations occurring just steps away from patient scans are among the reasons that the pace at which new MRI technology becomes available for clinical use is often compressed—translating into earlier and more effective diagnoses and treatments for patients at UH and around the world.
"What could be scar tissue might be interpreted as tumor regrowth because they both show up as a bright area in the image. But with MRF, tumor tissue is distinctly different from scar tissue." -Mark Griswold, PhD
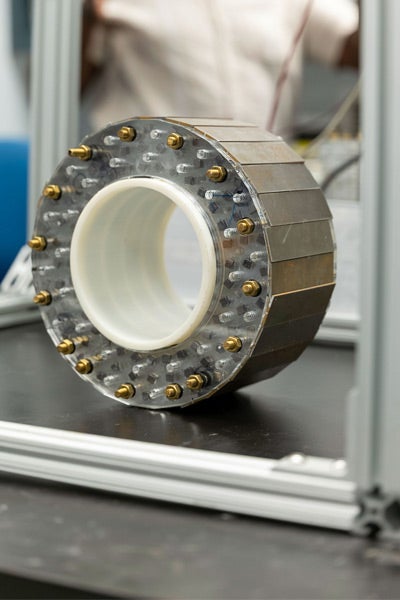
The lab also contains an engineering space where researchers are building prototypes of a new generation of MRIs that contain permanent magnets—requiring no electricity and, as a result, having the potential to become more accessible around the globe. Griswold co-leads a project funded by the United Kingdom-based Wellcome Foundation to design and send four such MRI machines to Uganda, Malawi, Nigeria and South Africa.
Such integration with the hospital and patients, Griswold said, “allows us to innovate on things that will have tremendous impact.”
Developing a clearer diagnosis
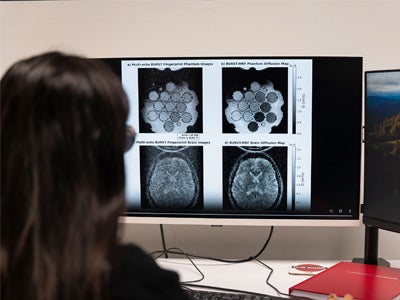
It was a Griswold-led team that made one of the most groundbreaking advances in the laboratory: the development of an entirely new way to characterize tissues using unique signal “fingerprints.”
They developed magnetic resonance fingerprinting (MRF) in 2013 by applying computational mathematics to magnetic resonance signals to quantify them with absolute numbers—akin to using a thermometer to take a temperature instead of feeling someone’s forehead.
While MRIs and MRFs can be performed on the same scanners, results of conventional MRIs produce images subject to interpretation, Griswold said. “What could be scar tissue might be interpreted as tumor regrowth because they both show up as a bright area in the image,” he said. “But with MRF, tumor tissue is distinctly different from scar tissue.”
MRF is approved by the U.S. Food and Drug Administration, available on all Siemens MRI machines and being used around the world. Researchers are currently using it in one UH clinical trial to assess the effectiveness of chemotherapy on breast cancers after just one week of treatment because clinicians can see previously undetectable changes in tumors. MRF also is being used in a CWRU-Cleveland Clinic trial involving a rare childhood kidney disease to test its ability to identify high-risk patients and measure disease progression with the hope of developing therapies.
And Griswold said the imaging center is doing preliminary studies with MRF that show the ability to track the progression of other diseases as well. “It has the potential,” he said, “to be transformative for both patient outcomes and healthcare costs.”


