Medical school graduation and the beginning of residency mark significant milestones in which dreams become reality, and high achievement and sacrifice often result in celebrations and rewards.
But earning the title of “doctor” also can be unnerving. Imposter syndrome can take hold of even the best-prepared students, but the “Transition to Residency” course, offered at Case Western Reserve University School of Medicine, is helping students combat that feeling.
The two-week, mostly simulation-based course, prepares students for their new roles as working physicians by placing them in highly realistic scenarios.

“Our goal is to have medical students who are very ready to take care of patients,” said Lia Logio, the John L. Caughey Jr. MD Professor of Medicine, vice dean for medical education and director of the Center for Medical Education. “So just before they become residents or interns in their respective specialties, this course is a good refresher and helps pull all of their learning together.”
The course evaluates student competency in a variety of areas, such as airway management, arrhythmias, seizures, shock, declaring death, completing a death certificate, giving bad news to a patient and their family, signing out from one provider to another, calling for a consult and more.
“There are going to be times where they are the only doctor in the room, “ said Andrew Golden, assistant director of the “Transition to Residency” curriculum and assistant professor of emergency medicine. “We want them to be prepared for those first five to 10 minutes, so we have based the curriculum around simulations to mimic
the crises they will experience while on call.”
In 2023, Golden and fellow University Hospitals emergency room physician Matthew Stull spearheaded the well-received “Transition to Residency” pilot. The course (like the pilot) relies heavily on the high-fidelity manikins and spaces in the Clinical Skills and Simulation Center (Sim Center) located on the Health Education Campus.

Daniel Salcedo, director of simulation and educational technology for the School of Medicine, said the course allows students to merge theoretical knowledge with the practice of caring for patients.
“We create conditions that are very close to what would happen in a real patient and engage learners in responding to those conditions,” said Salcedo.
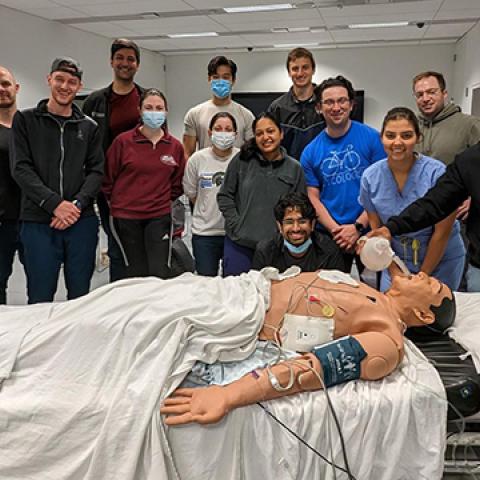
The Sim Center manikins breathe and blink, have beating hearts and life-like skin, and react like humans. For example, when positioning the head for intubation, the manikin’s head and jaw move and respond to handling realistically—and the airway is just as accurate on the inside. In addition to intubation, the manikins allow students to practice defibrillation, punctures with syringes and scalpels and more. The Sim Center team even develops recipes to replicate bodily fluids that ooze and emit on cue.

The Sim Center spaces transform to look like operating rooms, emergency room bays and outpatient exam rooms. They include monitors that display manikin patient data, crash carts, defibrillators, intravenous machinery and even paid professional actors who serve as family members and patients.

“It feels like real life, and you get that same adrenaline rush, that same deer-in-the-headlights feeling,” said Anastasia Rowland-Seymour, associate dean of program innovation and educational enhancement at the Center for Medical Education and associate professor of internal medicine.
Preceptors and instructors observe students using two-way mirrors, cameras and microphones and determine the manikin’s physical conditions in the control center. As students choose treatment options, the manikin responds realistically.
“It’s a fairly high-stress situation, “ said Rowland-Seymour. “If they don’t come up with a broad enough differential diagnosis and misdiagnose the patient, they have to deal with the consequences.”
Logio said doctoring is both an art and a science, and being productive in those emergent settings is crucial because efficiency matters in real life.
Salcedo said true learning happens when students forget they are in a simulation, adding, “it’s a little bit of magic.”
Learning from mistakes
The course only becomes effective when students debrief to discuss both successful and challenging aspects of the simulation.
Working in small groups of 15 to 16 learners, every course participant gets an opportunity to take the “hot seat,” but they also learn from one another.
“The student providing feedback is also learning because they’re thinking, ‘If I were in that situation I would have done such and such,’” said Rowland-Seymour.
The team says most students are very competent but lack confidence.
“It’s about giving students the ability to measure their own confidence through reflection and then applying that reflection in a way that allows them to understand what areas need to be improved for them to perform better,” said Salcedo.
What’s next?
A self-described “tech geek,” Salcedo said he looks forward to advancements in augmented reality, virtual reality and artificial intelligence—specifically more complex robots and deeper data interpretation.
The “Transition to Residency” course runs April 8–19. The school is expanding the program, as it will be mandatory for all fourth-year students in 2025.
“The feedback we got from students last year was really stellar, and we’re hoping the course continues on that trajectory,” said Golden.
School of Medicine alumnus and “Transition to Residency” pilot participant Peter Ahorukomeye—a resident in the Harvard Combined Orthopaedic Residency Program—took to Twitter/X recently to thank professors for a diagnostic tool he learned in the course.

“It’s sort of a mantra we instill in students: When you don’t know what to do, fall back on the basics—IV, O2, monitor and a new set of vital signs,” said Golden of Ahorukomeye’s post.
“The pace of work in a U.S. hospital is considered the most complex work environment known to man,” said Logio. “‘Transition to Residency’ gives students an opportunity to practice and hone their skills so they are ready when most residencies begin July 1.”